
In the strategic architecture of a personal injury case, the medical treatment phase functions as the primary evidentiary engine. When this phase is left to the patient’s own navigation, the resulting lack of structure creates profound administrative and valuation risks that are often irreversible by the time of demand. The presence of unmanaged personal injury treatment fundamentally compromises the narrative of a claim by allowing for evidentiary gaps, inconsistent documentation, and behavioral signals that insurance adjusters use to devalue the litigation.
Strategically, a case without professional coordination suffers from a lack of “medical-legal alignment.” Without an authoritative oversight layer, the clinical record becomes a collection of fragmented encounters rather than a cohesive story of causation and damages. This lack of case architecture not only complicates the attorney’s work during the demand phase but also signals to the insurer that the claim lacks the structural integrity necessary to withstand rigorous defense scrutiny.
The following analysis explores the specific administrative vulnerabilities inherent in unmonitored treatment pathways, from initial intake failures to the internal valuation modeling used by insurance carriers to suppress settlement leverage.
The Administrative Fragility of Initial Case Intake
The trajectory of a personal injury claim is often determined long before a demand is drafted. In the early stages, “evidentiary gaps” are frequently created when there is a mismatch between the patient’s clinical needs and the legal requirement for immediate, documented care. Within the context of unmanaged personal injury treatment, the most significant risk is the delay between the incident and the first medical evaluation.
Industry research and claims evaluation psychology suggest that adjusters view gaps in treatment as primary indicators of non-severity or intervening causation. When a patient is left to find their own specialists, they often encounter “administrative friction,” such as providers who do not understand Letters of Protection (LOP) or offices that lack the capacity for rapid intake. This results in:
- Behavioral Signaling: Unmonitored patients may inadvertently signal a lack of urgency, which adjusters interpret as a lack of genuine injury.
- Documentation Lag: Without immediate scheduling, the “acute” phase of the injury remains undocumented, allowing defense counsel to argue that subsequent symptoms are “degenerative” or “age-related” rather than traumatic.
- Intake Vulnerabilities: A structured intake must evaluate the mechanism of injury (e.g., occupant kinematics in a collision) early to determine the appropriate specialist pathway.
Structural Risks of Fragmented Coordination
Effective care coordination is a complex multidisciplinary effort that requires the management of “sequential” and “parallel” communication. In unmanaged cases, the lack of “cross-talk” between tertiary and primary care providers leads to what industry studies call “care fragmentation.” medical mismanagement in personal injury cases often manifests through a “paucity of handovers” between specialists.
For example, a patient may see a general practitioner who fails to identify the signs of a traumatic brain injury coordination or “hidden” orthopedic instability that requires advanced imaging. This lack of communication creates a clinical record that is inconsistent and easily picked apart during a deposition.
Managed vs. Unmanaged Pathways
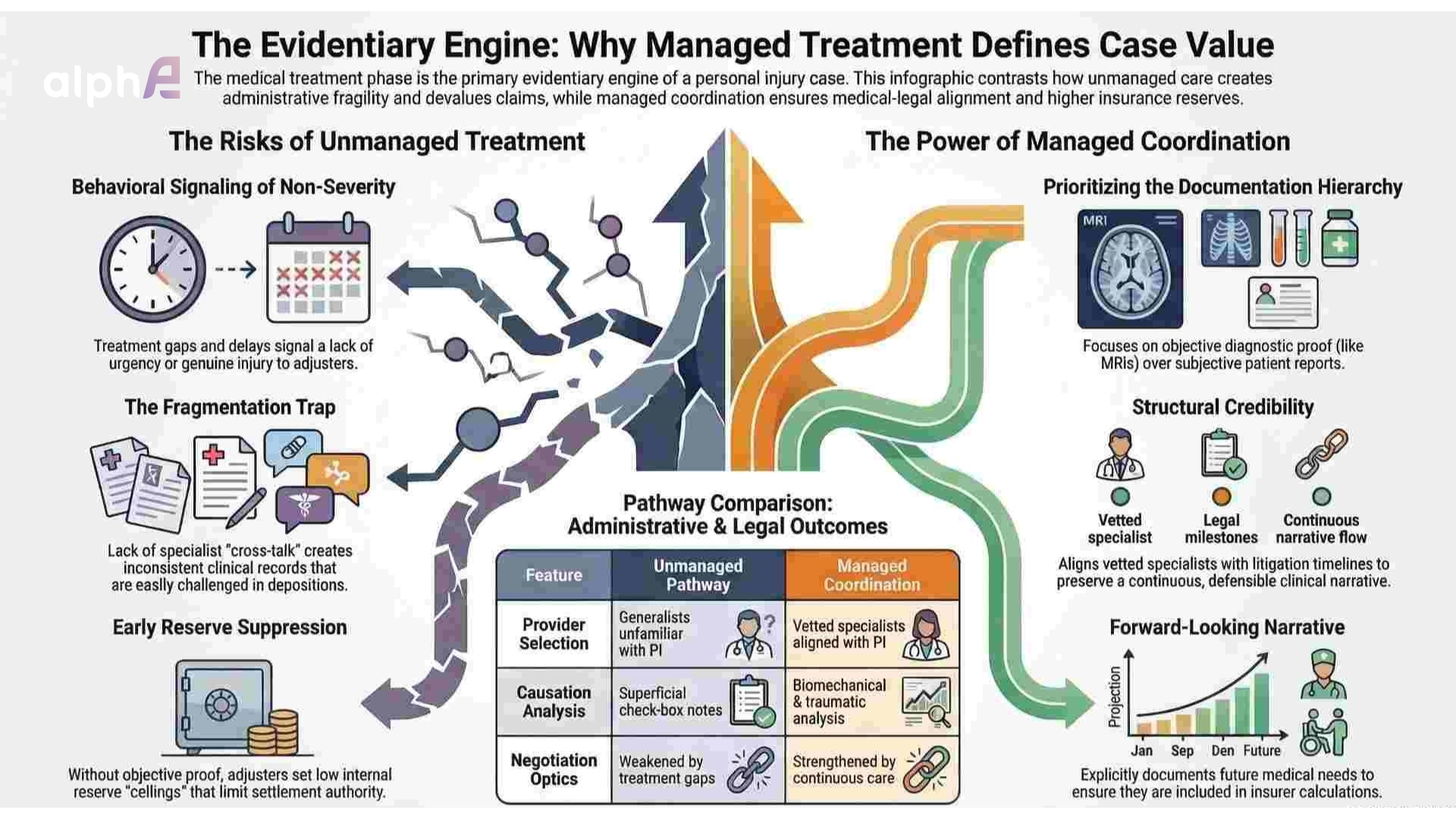
When comparing unmanaged and managed pathways, the structural differences directly affect case positioning and evidentiary weight.
In unmanaged treatment, provider selection often defaults to generalists unfamiliar with litigation dynamics, continuity of care is interrupted by treatment gaps, and imaging may be delayed beyond the acute diagnostic window. Communication typically relies on fragmented record transfer, while causation analysis is reduced to superficial, check-box documentation.
Managed coordination, by contrast, aligns vetted specialists with litigation timelines, preserves a continuous clinical narrative, prioritizes timely diagnostics, and integrates biomechanical and traumatic analysis into the record. The cumulative effect is not merely clinical efficiency but structural credibility.
These risks associated with poor treatment coordination ultimately create documentation fatigue for the legal team, which must later reconcile inconsistencies that could have been prevented through oversight.

Positioning and the Documentation Hierarchy
In the legal arena, a medical record ceases to be a mere clinical tool and becomes a “factual foundation” for expert opinion. When PI treatment is not monitored, the “documentation hierarchy”, the prioritized order of evidence from objective diagnostic proof to subjective patient reports, often collapses.
Insurance adjusters and defense experts prioritize “objective proof,” such as high-resolution MRI or neurocognitive testing, over the “subjective information” provided by a patient with varying levels of health literacy. Without a managed pathway, a case may rely too heavily on subjective pain reports, which are easily challenged. medical mismanagement in personal injury cases frequently results in records that lack “authentication and verification,” making them difficult to admit as evidence.
To maintain strong negotiation optics, the documentation must reflect:
- Causation Clarity: Explicitly linking the clinical findings to the “mechanics of the accident.”
- Longitudinal Tracking: Showing how symptoms like those from orthopedic trauma or spinal disc pathology evolve and persist over time.
- Future Requirements: Documenting the likelihood of future medical needs, such as hardware removal or revision surgeries, which are essential for calculating long-term damages.
Insurer Interpretation and Internal Valuation Modeling
A critical but “hidden” aspect of the claims process is the setting of insurance reserves. Once an insurer is notified of a potential claim, the adjuster must “set the reserve”, an internal budget and financial obligation on the balance sheet. This number often serves as the “ceiling” for settlement authority.
Insurance carriers use statistical methods and historical data (such as the “Chain Ladder method”) to project the ultimate cost of a claim. Adjusters are incentivized to keep these reserves as low as possible because “money held in reserve is far less profitable” for the insurance company. What happens when PI treatment is not monitored is that the adjuster lacks the “credible proof” required to raise that reserve early in the process.
Behavioral Signaling and Reserve Impact
Insurance evaluation psychology places significant weight on “credibility” and “impression.” If an unmanaged patient makes administrative mistakes, such as discussing prior injuries prematurely or minimizing symptoms to a friendly adjuster, the insurer will use that information to lower the reserve.
- Open Reserves as Liabilities: Carriers have a financial incentive to close appropriately valued files to release the reserve back into their general fund.
- Settlement Authority: Most adjusters will not settle for an amount in excess of the reserve, as doing so admits a failure in their initial duty to set an accurate budget.
- The Valuation Gap: In unmanaged personal injury treatment, the insurer may never see objective imaging or “specialist notes” that would compel them to increase the reserve, leading to “lowball” offers that cannot be negotiated upward without the expense of a trial.
Valuation Impact and Negotiation Optics
The final valuation of a personal injury case is not just a sum of the medical bills; it is a reflection of the “credibility weight” of the evidence. risks associated with poor treatment coordination include the creation of “treatment gaps,” which adjusters use to argue that the patient recovered or that a later event caused the pain.
In the context of medical mismanagement in personal injury cases, the negotiation optics are weakened when the documentation is disorganized or incomplete. For high-value claims involving spine care or neurology, the “preponderance of evidence” depends on a continuous care timeline. If this timeline is broken due to a lack of oversight, the settlement leverage evaporates.
Future Care Projections and Structural Undervaluation
What happens when PI treatment is not monitored is that future care projections, which often drive the most significant portion of case value, are frequently omitted. A valuation model cannot account for risk that is not documented.
For example, a complex fracture may lead to early-onset arthritis, but if the treating physician does not explicitly document this traumatic mechanism and the need for future intervention, the attorney has no basis to demand compensation for it. The absence of forward-looking medical narrative does not eliminate the risk; it simply removes it from the insurer’s calculation framework.
At alphae, this structural gap is analyzed from a positioning perspective rather than a clinical one, focusing on how documentation hierarchy and case architecture influence negotiation optics. Attorneys seeking further analytical insight may connect with our team through this page.
Conclusion
The risks of unmanaged personal injury treatment are not merely clinical; they are structural and financial. When a case lacks “litigation-ready” documentation and a managed specialist pathway, the “evidentiary engine” stalls. Insurance adjusters exploit the inconsistencies and gaps inherent in poor treatment coordination risks to set low internal reserves and suppress valuation.
Ultimately, what happens when PI treatment is not monitored is the loss of strategic control. For attorneys, ensuring “medical-legal alignment” from the first referral is the only way to build a “persuasive, defensible case” that maximizes settlement leverage while minimizing administrative friction. Strategic oversight ensures that every medical record serves its ultimate purpose: providing the objective, authenticated proof required for a successful resolution.