ER records personal injury claim documentation is often the first medical proof a firm receives, but it is also one of the most overestimated parts of the file. The client went to the emergency room, a clinician documented the visit, and the file has a diagnosis to point to. The trouble is that an emergency department note is written to answer a clinical question, not a legal one.
That single visit exists to decide whether someone is safe to discharge, not to track an injury through recovery. So while the record confirms the client was hurt and treated, it says little about how serious the injury became, what care followed, or whether there is a continuous medical story behind the claim.
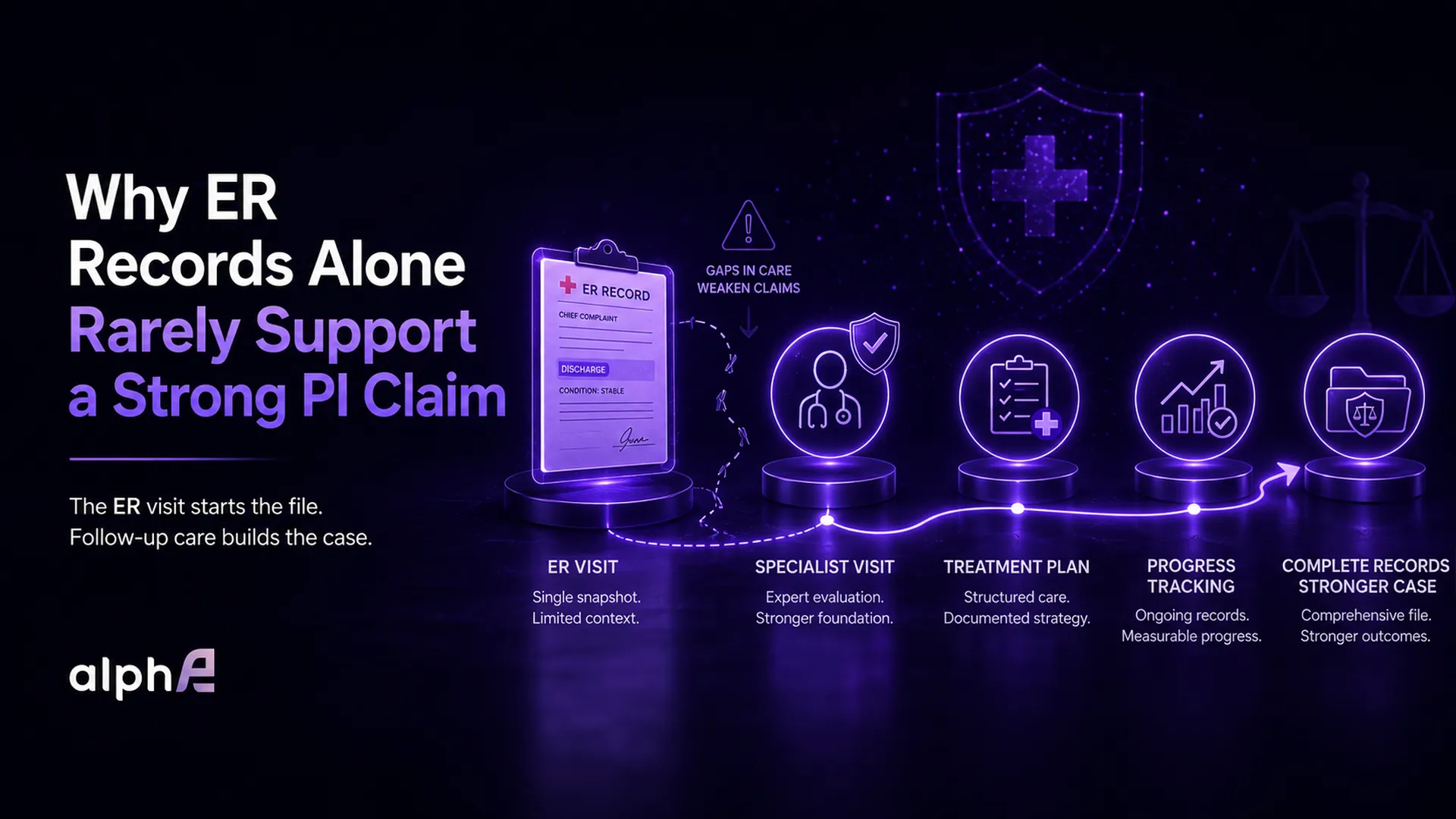
This article breaks down what an emergency department note actually contains, the two places it stops short in a PI claim, and what has to happen in the weeks afterward to turn that first visit into documentation a claim can stand on.
What Emergency Room Records in a Personal Injury Claim Are Built to Do
An emergency department note is organized around the acute encounter. It captures the chief complaint, vital signs, the imaging or labs run that day, a working diagnosis, and a discharge plan. Every field serves one purpose: deciding whether the patient can safely go home.
That purpose is also the boundary. For car accident injury cases, where the emergency room is frequently the client’s only medical contact in the first week, those limits matter even more. The visit is fast and triage-driven, so ER records reflect a first impression formed under time pressure, not a considered assessment of how an injury will behave over the following months. Anything outside the safe-to-discharge question tends not to make it into the chart: the detailed mechanism of injury, the prognosis, the plan for ongoing care. Those are the elements a claim leans on, and they are the elements an emergency visit is least equipped to provide.
Why Severity Often Reads Low at Intake
Two things flatten the picture early. Adrenaline and shock mute pain in the hours after a crash, so the level a client reports in the ER is frequently lower than what they feel two days later. And many injuries, such as disc involvement, joint damage, and post-concussive symptoms, have simply not declared themselves yet.
The result is a note that can describe a serious injury in mild terms. That is not a mistake by the treating clinician. It is an honest record of a moment that came before the injury fully developed, which is exactly why it reads differently from the specialist records that follow.
Where ER Records Stop in a PI Claim
Two specific gaps matter most when a claim is reviewed later.
The first is causation. An emergency department note documents what the client reported and what the clinician observed, but it is not written to tie the injury to the event the way a claim eventually needs. A line reading “patient reports neck pain after a motor vehicle collision” records a complaint and a context, not a medical opinion connecting the two. An adjuster reading only that line can fairly ask what evidence links the injury to the crash, and ER records on their own rarely answer the question.
The second is the treatment arc. The note ends at discharge. Everything that gives an injury weight, including the specialist evaluation, the imaging read, and the course of therapy, lives in records created later, by other providers. That is the core limitation of ER records personal injury claim documentation: it starts the medical timeline, but it does not complete the story of causation, severity, or treatment.

Discharge Instructions Are Not a Treatment Plan
A discharge summary tells the client what to do next: see a specialist, rest, return if symptoms worsen. It records intent, not follow-through. A treatment plan that is built, scheduled, and carried out through specialist care is what shows the injury was serious enough to pursue. When a file holds the instruction but no proof it was acted on, the gap reads as a recommendation the client set aside.
Why the Weeks After the ER Visit Decide the Claim
An unexplained stretch between the first visit and the next provider is where a PI claim quietly weakens.
The most consequential part of an ER-based claim is often not in the note at all. It is in what happens, or fails to happen, in the days that follow.
A familiar pattern: the client is discharged with instructions to follow up, then goes quiet for three or four weeks before seeing anyone else. On the file, that reads as one visit and a long silence, and a reviewer has little reason to interpret the silence as anything but a minor injury that resolved on its own.
Firms that understand the cost of inconsistent follow-up care treat that interval as the real exposure. The injury can be genuine and the silence entirely innocent. A client may be juggling work and childcare, or a scheduling call may have gone to voicemail. But with no documentation, the record cannot say so. The gap, not the visit, is what the firm has to manage.
How ER Records Become Strong PI Claim Medical Documentation
Closing that exposure comes down to continuity: a record that moves from the first visit to specialist care to resolution without an unexplained break in the middle.
A claim with that continuity reads in sequence: injury, emergency evaluation, prompt specialist follow-up, a documented plan, and notes showing the client carried it out. The entry that began as a single line in an ER chart becomes a tracked condition with a clear course and a visible cause. That is what a clean PI claim medical documentation trail looks like in practice. It also closes the openings a defense leans on, such as the claim that the injury was pre-existing, exaggerated, or unrelated to the event, because each is answered by a dated record rather than a later explanation.

How Follow-Up Care Strengthens an ER Records PI Claim
The follow-up visit is where the gaps from intake usually get filled. A specialist has what the emergency department did not: time to examine, image, and form an opinion. That is where the link between the event and the injury actually gets written down, and where severity is finally assessed against a fuller picture.
A specialist who sees the client soon after the initial visit can connect the dots in the chart, recording what the injury is, its likely cause, and the plan to treat it. A connected note like that carries far more weight than a first impression formed in triage.
How Coordination Keeps the Record From Going Quiet
Continuity rarely breaks because the client refuses care. It breaks because no one owns the handoff out of the emergency room. The discharge instruction goes to someone who is hurt, distracted, and unsure what to do next, and then nothing prompts the step that matters.
Treating that discharge as a handoff rather than an endpoint changes the outcome. It becomes a trigger: confirm the referral, help book the specialist, and verify the appointment was kept. A standardized referral handoff keeps that transition moving even when follow-up depends on a provider willing to treat on a lien. None of it pressures the client. It simply makes sure the days right after discharge are tracked instead of lost.
The Same Injury, Two Different Files
The same injury can produce a disjointed file or a continuous one, depending on what follows the first visit.
Two clients leave the same emergency room after the same rear-end collision, both with neck and lower-back pain and identical discharge instructions.
The first is left to manage the follow-up alone. The referral sits unconfirmed, a scheduling call goes unanswered, and twenty-three days pass before an orthopedic visit. The chart shows an ER note, a three-week void, then a late specialist entry that has to reconstruct the story from memory.
The second client’s discharge is handled as a handoff. The referral is confirmed within two days, the orthopedic exam happens that week, an MRI is ordered and read, and the therapy plan is documented as it unfolds. Same collision, same injuries, but one file argues for itself and the other needs explaining.
Frequently Asked Questions About ER Records in PI Claims
What do ER records prove in a personal injury claim?
ER records prove the client sought care and capture the immediate clinical findings, including the complaint, vitals, same-day imaging, and a working diagnosis. What they generally do not establish is causation or the long-term severity of the injury, which is why they work best as the opening entry in a fuller record.
How soon after the ER should a client see a specialist?
Sooner is better, for treatment and for the file. There is no fixed deadline, but a long, unexplained stretch between the emergency visit and the next provider is the single thing most likely to make a real injury look minor on paper.
Can a personal injury claim succeed with only ER records?
It can, but it is rarely the strongest position. A claim built on one visit asks a reviewer to infer everything that came after. Continuous follow-up documentation removes the guesswork and gives the claim a record it does not have to defend.
Why do emergency room notes sometimes understate an injury?
Adrenaline and shock can mask pain right after an accident, and some injuries take days to present. The note honestly captures the moment, but the moment is often before the injury has fully developed.
Final Takeaway
An emergency room visit is a strong place for a personal injury claim to start and a weak place for it to stop. ER records fix the moment of injury in the file but say little about cause, severity, or recovery, the parts a claim is ultimately judged on.
The practical move for a PI firm is to treat the ER discharge as the first link in a chain, not a finished exhibit: own the handoff, confirm follow-up happens, and keep the medical timeline unbroken so no silent stretch has to be explained later.
alphaE helps Texas PI law firms strengthen documentation beyond the emergency room by coordinating follow-up referrals, supporting scheduling visibility, tracking treatment communication, and confirming medical records follow-up from the emergency room visit through settlement review.